This information leaflet is for patients who are having an examination of the bowel (known as a colonoscopy). The leaflet explains the reasons for the examination, what is involved, and about any possible risks or side effects.
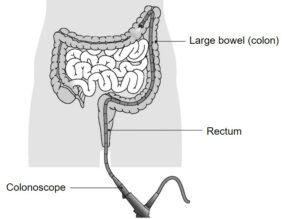
A colonoscopy is an examination of the inside of the large bowel using a long flexible instrument called a colonoscope. This is introduced into the colon via the back passage and an image is projected via a small camera onto a screen.
Reasons for having this examination include:
- To investigate your symptoms. The results can help us to decide on the best treatment for your problem or whether we need to carry out further examinations
- To treat abnormalities such as polyps
- To re-examine any previous problems
What is a polyp?
A polyp is a protrusion from the lining of the bowel. If a polyp is found, or if we already know you have a polyp, it is usually removed by the endoscopist as some polyps can cause problems in the future. Alternatively, your endoscopist may take some sample biopsies for further examination.
Preparation for the examination
For this examination to be successful your bowel must be as empty as possible. You will be given a laxative (instructions for this will be provided separately) and a recommended change in diet for a few days before the test. It is very important to follow these instructions carefully and drink plenty of fluids on the day before the examination.
Patients must not stop any prescribed medication including blood pressure tablets unless advised by your consultant. If you are however on any iron preparations or medication that may make you constipated, this must be stopped 7-10 days before your procedure.
If you have diabetes, or you are taking anticoagulants (blood thinning medication) such as warfarin, ticagrelor clopidogrel, dabigatran, rivaroxaban, edoxaban or apixaban, you will be given specific instructions in advance. Patients who continue to take Warfarin, or who have stopped Warfarin just before the test, will need to have a blood test on the day in the unit.
Please read and complete your medical assessment form in advance of your procedure. You will also be sent a consent form which a nurse will discuss with you on the day.
If you have not been advised what to do about your medicines or if you require any additional access or support, please call 07815 178199 Mon-Sat between 10:30 11:30am and 14:30-15:30pm only.
Outside of these hours, this telephone is for Emergency calls only.
On arrival at the hospital
- Please go straight to the Endoscopy Unit and ring the bell to let the staff know you have arrived
- Procedure times can be unpredictable so you may have to wait a while, it is a good idea to bring something to read
- A nurse will discuss your medical history with you, while also checking your pulse, blood pressure, oxygen levels, blood sugar (if diabetic) and clotting (if on anticoagulants). They will ask any necessary additional questions and you will have the chance to ask anything you may want to know
- The nurse will discuss the consent form with you to confirm that you understand the procedure and agree to go ahead with it, after which you should sign the form. You will be given an identity band which you should also check for accuracy
- You will then be asked to undress into a hospital gown. Put on your dressing gown over this and wait until you are taken through to the examination room
- A nurse will remain with you throughout the examination.
The examination
Most examinations last between 20 and 45 minutes. Not all procedures require sedation and some patients choose to have no medication or Entonox (gas and air).
If you choose to have sedation and/or a painkiller you will be given an injection to make you as relaxed and comfortable as possible. Sedation may also make you feel sleepy but for most patients it induces sleep after the examination, rather than during it. We will monitor your heart rate and breathing throughout.
In order to have sedation and/or pain relief it is important that you have a responsible adult to look after you for 24 hours after your colonoscopy. As an alternative you may be offered Entonox, an inhaled painkiller. Throughout the test you also may be given oxygen via a nasal tube.
While you are lying comfortably on your left side on the examination trolley, the doctor or nurse specialist will gently pass the small flexible tube (colonoscope) into your large bowel via the back passage.
Some air is passed into the bowel to expand it to allow for a clear view. This can cause some discomfort but it will not last long. You may feel as if you want to go to the toilet but be reassured that this will not happen. Most of the air will be sucked out at the end of the test.
The bowel can be very long and bendy, so manoeuvring the tube around it can take time and may cause some discomfort and stretching. In order to complete the examination it is occasionally necessary to change your position onto your front, back or right side. An assistant may have to press on your abdomen to assist the procedure. Air that has been passed up into the bowel will have to come out again as wind. Please do not worry about this, it is quite normal.
A biopsy (a small sample of tissue) may be taken during the examination to be sent into the laboratory for further tests. This does not cause pain.
Occasionally polyps are found in the bowel and can be removed. This again is painless but can result in bleeding from the lining of the bowel when the polyp has been removed. This bleeding usually settles down quickly.
After the examination
If given sedation or a painkiller injection, you will be taken to the recovery area. Once recovered from the effect of the sedation and the procedure, you will be offered a drink and a biscuit.
A nurse will explain the findings of your procedure and you will be given a copy of your report before being discharged. It would be a good idea for an adult member of your family or a friend to be present as you may not remember everything you have been told.
You may experience some more discomfort from wind – this should settle after a few hours.
The sedative effects (if administered), may make you sleepy and can last for 24 hours. Even though you may feel alert you must be accompanied home. If you had the sedative injection and/or analgesia, you must have a responsible friend or relative to take you home and stay with you for 24 hours. If this is a problem, please telephone the department as soon as possible. For 24 hours post procedure you must not drive a car, drink any alcohol, sign any legally binding documents or operate machinery.
Individuals are unable to donate blood for 4-6 months following any endoscopic procedure. (British Society of Gastroenterology guidance; updated February 2020).
The risks
Colonoscopy is a safe procedure but there can be a risk of the following:
- Bowel preparation can cause immediate problems with the kidneys, particularly in patients with known kidney problems or those who are on medication that affects the kidneys. This can usually be treated, however very rarely there may be permanent damage.
- A tear (perforation) in the lining of the bowel: Nationally this happens to approximately 1 in 1000 people. The risk of a tear is higher with polyp removal. If we know before your colonoscopy that you have a large or difficult to remove polyp, your endoscopist will discuss the risks with you in more detail. An operation may be required to repair a tear if it cannot be closed during the colonoscopy.
- Risk of missed lesion: Although colonoscopy has been selected as the best test to diagnose your symptoms, no test is perfect. There is a risk of 1 in 100 that we might miss a large polyp or other important finding during your test.
- Bleeding where we take a sample (biopsy) or have removed a polyp: Happens to around 1 in 100 people, but this is usually minor and often stops on its own.
- Short term problems with breathing, heart rate and blood pressure (related to sedation): 1 in 100. We will monitor you carefully so that if any problems do occur they can be treated quickly. Older people and those with significant health problems (for example, people with serious breathing difficulties) may be at a higher risk.
- Heart attack or Stroke (related to sedation): 1 in 5000.
Women taking the oral contraceptive pill should be aware that taking bowel preparation might prevent the absorption of the pill. Additional contraceptive precautions should be taken until the next period begins.
If you have any concerns about these risks please talk to your specialist before your colonoscopy.
Alternative procedures
The main alternative is a CT scan; however this is not as accurate as a colonoscopy, biopsies cannot cannot be taken and procedures cannot be performed with x-rays and scans.
Air travel
If you have had a diagnostic procedure, you would be advised not to fly for 48 hours after your procedure. If you have undergone a therapeutic procedure, you should not undertake any air travel for 2 weeks after your procedure. You will be advised on discharge which procedure you have had.
Sleep Apnoea
Please bring your CPAP machine with you for your appointment because if you choose to have sedative injection, due to the possible side effects, it might be necessary for it to be used to ensure your safety.
Pacemaker Device or Implantable Cardioverter Defibrillator (ICD)
Please bring your pacemaker device or implantable cardioverter defibrillator manufacture information card with you a cardiac technician might be required and will need that information to make sure your device is safe for you during this procedure.
Additional Information
What is Entonox?
Entonox is the trade name for the mixture of 50% Oxygen and 50% Nitrous Oxide, also known as ‘gas and air’. It is a fairly strong pain killer which works very quickly. It is often used to treat pain during childbirth, trauma and wound care. An advantage of this method of pain relief is that it is fully removed by the lungs within a few minutes after you have stopped breathing it. Entonox is safe for use in pregnancy and breastfeeding mothers.
How does Entonox work?
The exact way Entonox works is not fully understood. It is believed that once it is inhaled, Entonox travels to the brain and the spinal cord where it stops the pain from being felt.
Why is Entonox used during endoscopic procedures?
Endoscopic procedures such as flexible sigmoidoscopy and colonoscopy involve the passage of a smooth, flexible tube which has a camera on the tip, into the bowel so that the lining can be inspected. In order that the Endoscopist can view the lining, it is necessary to introduce air into the bowel through the endoscope. This can be uncomfortable and even painful for short periods. Inhaling Entonox can help to make these procedures more manageable. It may be used on its own, or in addition to intravenous (injected) sedation and analgesia if required.
What are the benefits of using Entonox?
Entonox is an effective analgesic (painkiller) which also has sedative and amnesic effects. This means that in addition to relieving pain when used for short periods, it makes the user feel temporarily drowsy, and reduces the memory of the uncomfortable experience. Entonox puts you in control of your pain relief, because it is self-administered.
Entonox wears off quickly, starting to leave your system as soon as you stop inhaling it. It has very few, mild side effects and leaves the user fit to drive within half an hour after it is last used. This can make Entonox an attractive alternative to injected sedation for those who have commitments such as work or childcare to consider.
Entonox works quickly; you may begin to feel some effect after your first few breaths. It normally takes about two minutes for Entonox to begin to work. After inhaling the gas for a couple of minutes, effective levels of pain relief should be experienced to help you cope with the discomfort of your procedure. The nursing staff will support you in the safe, continued use of Entonox as you require it during your Endoscopy.
How is Entonox given?
The Endoscopy nursing staff will show you how to use the Entonox effectively and monitor and support you while you are using it. Before your procedure begins, you will be given a mouthpiece which is attached to a cylinder of Entonox gas. It is important that you hold the mouthpiece firmly between your lips to form a good seal. The nurse will moisten your lips if they are dry to help you do this. You will need to breathe deeply for one to two minutes before there is enough Entonox in your body for it to work. Entonox will only flow when you breathe in, therefore the deeper you breathe, the better your pain relief will be. You do not need to breathe Entonox for your entire procedure; only at times of pain or discomfort.
What are the risks of using Entonox?
Entonox should only be used when prescribed by a healthcare professional. There are minimal risks associated with its short- term use. If it is used repeatedly or continuously for long periods (> six to eight hours) it can affect the user’s blood count, leading to anaemia or vitamin B12 deficiency, or reduce bone marrow function. These problems are very rare and not applicable in this setting.
When Entonox is used for short periods, the main concern is that the gas may become trapped in parts of the body. This is only likely to cause problems for those with specific medical conditions. The nurses will ask you for details of your medical history and carefully assess whether it is safe for you to use Entonox. You should not use Entonox if you have:
- A recent or current ear infection, or an operation on your ears
- Recent eye surgery where injections of gas have been used
- Recently been scuba diving (within 48 hours) or have decompression sickness
- A collapsed lung or pneumothorax
- Lung disease or breathing difficulties (unstable asthma, emphysema)
- A head injury (or suspected or known increased pressure on the brain)
- A known problem with air trapped in the body (e.g., in an artery)
- A severely bloated stomach
- Injuries to the face and jaw
- Paraquat poisoning (a weedkiller)
What are the side effects of using Entonox?
Entonox can make you feel dizzy or nauseous (sickly) but these side-effects usually settle if you slow your breathing down or stop using the gas. Some people complain of parasthesia (a tingling sensation) and light-headedness while using the gas.
If you keep breathing Entonox continuously, you will eventually become drowsy and unable to hold the mouthguard to your lips. The nursing staff supervising you will give you some oxygen while the effects wear off, and you will wake up naturally as this happens.
Use of Entonox will also be discontinued if you start to complain of earache, if you find the side-effects unpleasant or persistent, or if you are not finding it helpful, in which case alternative pain-relieving medication may be used.
Are there any restrictions after using Entonox?
You will be monitored for half an hour after you have stopped using Entonox, until the nursing staff are happy that you have recovered and are safe to be on your own and resume your normal activities, such as driving and working.
Endoscopy Training at Luton and Dunstable Hospital
Luton and Dunstable Hospital contributes to the training of endoscopists and as a result has several trainees working in Endoscopy; this leaflet is provided to inform you about how this
may affect your Endoscopy procedure, and support your decision as to whether you are happy to have a trainee perform the procedure.
Although the idea of a trainee may be unnerving it is often a very positive experience. All our Endoscopy trainees are in a structured training programme within the national guidelines.
Will they be supervised?
Under no circumstances are trainee Endoscopists unsupervised. Depending on the experience of the trainee, an experienced Consultant will be present, and supervising your Endoscopy procedure throughout or will be immediately available in the Endoscopy department. If at any time you or the trainee has any difficulties the trainer can intervene. All the Endoscopy trainers at Luton and Dunstable Hospital are accredited Endoscopy trainers and we regularly monitor their training skills.
Is it safe?
We carefully monitor our complication rates for Endoscopy and there is no difference in safety with a trainee Endoscopist.
Will it be more uncomfortable?
We carefully monitor patient comfort and have not found any suggestion it will be more uncomfortable.
Will it take longer?
While learning a trainee may be slower than an independent Endoscopist, however, our trainers are experienced in monitoring the length of a procedure and will take over if procedure seems prolonged. On a training list we allow a longer time for the whole Endoscopy experience, and patients often find this makes for a more relaxed atmosphere.
What should I do if I don’t want a trainee?
If you wish to let us know you are not happy to have a supervised trainee perform your procedure please inform us at least one week in advance of the procedure, so we can ensure you are not booked on a training list. The Endoscopy Booking Office can be contacted on 01582 497273.
For further information
For any medication queries please telephone 07815 178199
Mon- Sat between 10:30–11:30am and 14:30–15:30pm only.
Outside of these hours, this telephone is for Emergency calls only.